Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
4 Introduction to Wellness Tourism
Learning Objectives
This chapter provides a definition and description of wellness tourism and related forms of niche tourism. It also describes types of wellness resorts and retreats in the United States, within their historical context.
At the conclusion of this chapter students will be able to:
Wellness tourism is a mid-20th century phenomenon that has blossomed into a lucrative and fast growing sub-sector of the global wellness industry. While the sub-sector is by no means short of definitions, in practice it can be difficult to demarcate for reasons touched upon below. But first let’s consider two definitions by prominent industry organizations. The first of these is focused on the demand-side (the tourist) and the second focuses on the supply-side (those businesses that provide tourism products and services).
The Global wellness Institute (2023) defines wellness tourism as: Travel associated with the pursuit of maintaining or enhancing one’s personal well-being.
The Wellness Tourism Association defines wellness tourism as: A specific division of the global tourism industry that is defined by the common goal of marketing natural assets and activities primarily focused on serving the Wellness Traveler and those who want to be.
As both the supply and demand sides have a part to play in the wellness tourism equation, for the purposes of this course we will combine these definitions as follows:
Wellness Tourism Definition
Wellness tourism is travel for the primary purpose of maintaining or enhancing holistic well-being, along with the segment of the global tourism industry that caters to wellness travelers.
definitional issues in wellness tourism
In addition to the above, a plethora of other industry and academic definitions have been proposed and a sample of the latter is included in Table 2. While academic definitions are instructive, shedding light on how wellness tourism has been understood and interpreted by scholars and researchers, they also reveal some of the inherent difficulties in delineating wellness tourism as a sub-sector (see below).
Table 2: Academic Definitions of Wellness Tourism
Travel or leisure?
Carrera and Bridges (2006) offer a definition that describes travel as occurring outside one’s local environment. In the same vein, early academic definitions often specified that tourism should include an overnight stay (Smith, 1988), the crossing of an international border, or travel beyond a minimum radius—roughly 75 miles (Yu, Kim, Chen, & Schwartz, 2012). These criteria were introduced to distinguish tourists from residents engaging in local leisure activities, such as visiting museums or dining at neighborhood restaurants. However, because such criteria ultimately proved arbitrary, they have largely fallen out of use. The World Tourism Organization (UNWTO) now defines tourism simply as “the activity of visitors” (2008). The crux of this distinction resurfaces, however, when attempting to classify wellness-related activities within the scope of tourism. Consider day spas versus hotel spas: a local day spa frequented by tourists during the high season is not typically classified as part of the wellness tourism industry, whereas a hotel spa is, even if it also caters to local residents.
Holistic and purposeful
We often see definitions that reference the active pursuit of holistic well-being, in keeping with broader wellness definitions (see Wellness Definition in Chapter 1: The Wellness Revolution). For wellness tourism, the primary motivation or purpose of travel is further relevant because, on one hand, tourism is widely regarded as inherently beneficial, and on the other, travel is often undertaken for a variety of reasons. Findings from numerous studies support the idea that, in addition to decreased stress, burnout, and exhaustion, post-travel outcomes may include positive effects on perceived happiness, quality of life, and even physical health (Chen & Petrick, 2013). Wellness tourism thus distinguishes itself as the pursuit of holistic well-being as a primary purpose of travel. Tourists, however, may spend only part of their vacation in the active pursuit of well-being, while otherwise engaging in a variety of tourism activities. This has prompted the classification of travelers into primary and secondary wellness tourists, which will be discussed in Chapter 7: The Wellness Tourist (see “Who is a Wellness Tourist?”).
All wellness tourism is a form of travel but not all travel is a form of wellness tourism
While wellness tourism is often defined as a form of travel, it is not represented at every stage of a journey, nor is it strictly speaking a mode of travel, except in the case of wellness cruises. For example, a flight and an overnight stay at a standard hotel en route to a wellness resort may be part of the overall wellness tourism journey, but a traveler would be hard-pressed to wrestle any semblance of well-being from either experience. Thus, for the purposes of this course, we will distinguish between general travel services and wellness tourism services, in other words those catering specifically to holistic well-being (see Chapter 5: The Wellness Tourism Industry).
Related forms of niche tourism
Niche tourism is a term used to describe specialized or unique travel experiences, such as wellness tourism. It contrasts with mass tourism in that it involves smaller-scale sub-sectors centered around specific activities or areas of interest, typically pursued by distinct travel segments or interest groups. Several sub-sectors are closely related to wellness tourism. As depicted in Figure 6, such niche forms may be subsumed by (e.g., well-being tourism), overlap with (e.g., spa tourism), or be tangentially related to wellness tourism (e.g., medical tourism), as described below. These forms can also be arranged along a spectrum, ranging from those focused on physical well-being to those that are more psychologically or spiritually oriented.
Figure 6: Related Forms of Niche Tourism
Medical Tourism
Medical tourism, also known as medical travel, is defined as “contemporary travel for the primary purpose of obtaining indicated or elective dental or biomedical services” (Hudson & Li, 2012, p. 229). It is applied in the context of interstate, domestic, regional, or cross-border travel (including within the European Union) to receive medical, dental, or surgical care (Medical Tourism Association, 2024), though it is often used in an international context as well. According to the Medical Tourism Association, international medical tourism is now a $100 billion industry and is growing at a rate of 15% to 25% annually (2024).
The United States, with its strong pharmaceutical industry, research institutions, and high-tech medical facilities, was once a popular destination for inbound tourists seeking specialized care (Bookman & Bookman, 2007). In recent years, however, the flow has reversed, with medical tourism now characterized by outbound tourists traveling from wealthier, more developed nations such as the US to less developed countries for treatments ranging from complex procedures like cancer treatments to more routine care such as orthopedics, or elective services like dental and cosmetic surgery (Bookman & Bookman, 2007; Medical Tourism Association, 2024).
The initial impetus for this shift was the high cost of medical care, supported by the ease and affordability of international travel, rapidly improving technology, and international accreditation and the proven safety records of medical facilities in many developing countries(Bookman & Bookman, 2007; Medical Tourism Association, 2024). The touristic aspects of destinations further enhance the appeal, with travel companions and periods of recuperation often hosted in affordable luxury accommodations included in medical tourism packages (Bookman & Bookman, 2007). Medical tourists may also enjoy additional resources provided by destinations, such as favorable climates, beaches, heritage and cultural attractions, and gastronomy (Olta et al., 2023).
Persistent barriers to international medical travel include the availability and quality of post-treatment care, as well as financial concerns such as hidden costs or payment security (Medical Tourism Association, 2024). International accreditation serves as a crucial indicator of quality and trustworthiness for many patients considering medical tourism (Medical Tourism Association, 2024). Ethical issues also arise, particularly for treatments such as fertility procedures, organ transplants, stem cell therapies, and euthanasia, which can present additional complexities in international contexts (Lunt & Carrera, 2010). The impact of medical tourism on developing countries may raise moral dilemmas, as in Thailand, where the rise of hospitals catering to medical tourists led to an internal brain drain, reducing equity in healthcare access for local populations (Ramirez de Arellano, 2007).
While medical tourism is distinct from wellness tourism, the two have increasingly converged through increasing demand for elective procedures. Medical spas, also known as med spas or medi-spas, offer non-invasive or minimally invasive cosmetic treatments along with advanced skincare procedures and traditional spa services (Glow MedSpa, 2023). Medical spas, for example, may offer Botox, dermal fillers, laser hair removal, micro-needling, and CoolSculpting under the supervision of a licensed medical professional working alongside massage therapists and cosmetologists in a traditional spa setting (Glow MedSpa, 2023).
Health tourism
Health tourism is defined as “those types of tourism which have as a primary motivation the contribution to physical, mental, and/or spiritual health through medical and wellness-based activities” (European Travel Commission, 2018, p. 2). Thus, health tourism is an umbrella term that encompasses both medical and wellness tourism.
Thus, the evolution and utility of the term are best understood in a European context. Medical and alternative therapies, as we define them today, were once indistinguishable. In ancient Greece, for example, the potency of spring water was believed to restore the balance of humors (or bodily fluids), a concept grounded in astrology and central to Hippocrates’ medical practices and teachings (Tubergen & Linden, 2002). After a period of disuse during the Middle Ages, the 18th and 19th centuries saw a resurgence in the popularity of natural springs, around which both curative and wellness facilities developed (Olta et al., 2023). During this time, spas emphasized the medicinal properties of natural waters to treat a variety of ailments, such as skin diseases, digestive issues, rheumatism, and gout (Cohen & Bodeker, 2008). Spas were also visited for rest and rejuvenation, with most offering leisure activities and recreational amenities alongside traditional bathing rituals (Cohen & Bodeker, 2008).
It should come as no surprise then that medical tourism and spa tourism are traced to the same source in a European context (Mihalache, 2018), with echoes of these intertwined historical associations continuing to this day. Poland’s medical system incorporates therapeutic practices such as thermal baths, salt cave inhalations, and medicinal mud treatments, with origins dating back to the 13th century (Smith & Puczkó, 2014). German health insurance supports a range of treatments in hybrid medical and wellness facilities, while governments in Central and Eastern Europe provide medical subsidies for a number of prescribed wellness therapies (Smith & Puczkó, 2014).
Globally, and as with medical spas, the distinction between medical and wellness tourism has also begun to blur in wellness resort settings. According to the Global Wellness Institute (2023), the pandemic accelerated the merging of wellness and medical practices, with many diagnostics and procedures that were once exclusive to hospitals and clinics now being offered at destination spas and wellness resorts—such as lymphatic drainage, gut microbiome assessments, sleep analysis, blood tests, genetic testing, musculoskeletal assessments, and oxygen therapy (Global Wellness Institute, 2023). Concurrently, medical centers and hospitals have started integrating wellness practices into post-surgery recovery and rehabilitation, offering services like yoga, meditation, exercise, nutrition, energy healing, and bodywork, catering to both medical tourists and wellness seekers (Global Wellness Institute, 2023).
Spa Tourism
Spa tourism has been defined, simply, as “a type of tourism characterized by stays in a spa for the purpose of physical and mental rejuvenation” (Dimitrovski & Todorović, 2015). However, because the term “spa” is used in a wide variety of contexts to describe a range of treatment types and facilities, it is often framed differently depending on the context. In a European context, spa tourism tends to reflect its historical roots and has been defined as a type of tourism, “focused on the effect of relaxation and curative influence on the human body, achieved by the means of water-based procedures, such as mineral waters, thermal pools, vapor baths, and saunas. The emphasis is placed upon the healing properties, leading to recovery and renewal of the body” (Smith, 2008).
Spa tourism is considered a subset of wellness tourism (Dimitrovski & Todorović, 2015) as well as a subset of health tourism (Hall, 2012) because of its historical association with balneotherapy (cures through bathing) and, more recently, its association with medical spas that offer both wellness and elective medical procedures. The following comparison chart highlights distinctions between these closely related forms of tourism:
Comparison indicators of balneo, spa and wellness tourism (Georgiev & Vasileva, 2010)
Duration of stay
Motivation
Spheres of influence
Compulsory elements
Balneotherapy
Medium-term to long stays
Healing, prevention of health problems or existing disease
Physical state
Medical staff and supervision
SPA tourism
Short and medium-term stays
Body and mind renewal and re- energizing
Physical and mental without emotional state
Water-based and other procedures and/or treatments
Wellness- tourism
Medium-term to long stays
Optimization of health and overall well- being
Complex influence on the physical, emotional and spiritual state
Customized wellness programs prepared for any wellness tourist
The Global Wellness Institute (2023) identifies the spa industry as the most lucrative, largest, and most diverse sub-sector of the global wellness economy, in terms of the number and types of facilities. To reflect this diversity, it defines six categories of spas, as described in Table 3 below. Note that not all these categories (e.g. Day/club/salon spas) reflect types of tourism.
Table 3: Six Categories of Spa (Global Wellness Institute, 2023)
Spiritual Tourism
Spiritual tourism is defined as, “tourism which focuses on the secular spiritual domain of wellness using body-mind-spirit activities, retreats and ashram visits, and connection to nature and landscapes” (Smith & Puczkó, 2014).
While spiritual tourism may overlap with religious tourism, the two are not synonymous. Religious tourism centers on prescribed, traditional rituals and rites of faith, whereas spiritual tourism adopts a more eclectic and individualized approach to spirituality. Spiritual tourists often select or blend elements from multiple belief systems, creating personalized rituals and experiences that align with their desires, needs, or aspirations for personal growth, transformation, and meaning (Collins-Kreiner, 2020; Kujawa, 2017).
A defining feature of spiritual tourism is its experiential nature. Associated activities may include deepening a meditation practice, undertaking pilgrimages, visiting sacred sites, participating in shamanic ceremonies, or spending time in nature, each intended to foster introspection and spiritual growth (Kujawa, 2017; Rodrigo, 2020). Despite its focus on personal transformation, spiritual tourism frequently cultivates a sense of community through group activities, engagement with locals in spiritual traditions, and meaningful connections with like-minded individuals (Kujawa, 2017).
Described as a “quest for personal meaning from and through travel” beyond typical motivations such as leisure or recreation (Willson et al., 2013, p. 152), spiritual tourism is gaining popularity as travelers are increasingly seek authentic, purpose-driven experiences in a world often perceived as lacking depth and meaning (Halim et al., 2021). By 2000, an estimated 200 to 600 million people traveled annually for religious or spiritual purposes—half of them internationally (Olsen, 2016).
Pilgrimage
Pilgrimage is a popular form of spiritual tourism. Pilgrimages are journeys undertaken by foot to sacred places, edifices or shrines, for a variety of reasons such as a deepened connection to faith, spiritual growth, healing, penance, or to demonstrate devotion. While the practice dates to ancient times, organized pilgrimages became particularly prominent in various religions, such as Christianity and Islam, around the early Middle Ages. Today, however, an increasing number of people are undertaking pilgrimages for personal rather than religious reasons. In 2023, nearly half a million people walked the Camino de Santiago in Spain, one of the most famous pilgrimage routes (Turrell, 2024). Data from the Camino de Santiago Bureau of Registration showed that only 40 % of walkers were doing so for religious reasons (Turrell, 2024). Many undertake the Camino for physical and mental health benefits, self-discovery, or simply to live in the moment while surrounded by the cultural, historical, and natural beauty of such ancient pathways (Turrell, 2024). Along with record foot traffic along established routes, new routes have opened across the globe from the United States to Ireland, Bhutan, and Sri Lanka (Turrell, 2024).
Transformative tourism
Transformative tourism is defined as travel that “is part of the awakening of consciousness, and creates more self-awareness, more self-inquiry into the purpose of life, living by a higher set of values, and making greater contributions to others” (Sheldon, 2020, p. 2). Unlike other forms of tourism, transformative tourism is better understood as an approach to travel rather than a tourism sub-sector (Soulard et al., 2021). However, its principles strongly align with themes found in wellness tourism, and its growing relevance in both academic discourse and commercial practice merits brief exploration.
As both an empirical phenomenon and a prescriptive ideal, transformative travel may lead to enhanced well-being, expressed through feelings of fulfillment, curiosity, wonder, and personal growth (Pung & Chiappa, 2020). It further encourages introspection, heightened self-awareness, and existential inquiry, ideally serving as a vehicle for enhanced psychological and spiritual fulfillment (Soulard et al., 2021). Its objectives and potential outcomes are also closely linked to social and cultural sustainability—principles central to wellness tourism.
Transformation is a multifaceted concept, and there is no singular definition of what constitutes a “transformative” travel experience (Pung & Chiappa, 2020). Rather, transformative travel emphasizes the subjective experiences of travelers and the diverse ways in which travel can catalyze personal change (Pung & Chiappa, 2020). For some, this may involve developing greater self-efficacy by navigating challenges or unfamiliar settings. Others may experience transformation through emotional growth, the acquisition of new knowledge, and the creation of lasting, meaningful memories.
Facilitators of transformation may include overcoming challenges during a trip and immersing oneself in the local environment (Pung & Chiappa, 2020). Stepping outside one’s comfort zone—through language barriers, cultural differences, or unplanned circumstances—can foster personal growth and self-confidence. Truly appreciating a destination’s unique atmosphere, culture, and community can also prompt reflection, challenge perspectives, and foster a deeper appreciation for the diversity of the world.
Shared experiences, particularly those involving cultural immersion and emotional engagement, play a crucial role in creating transformative travel experiences. Opportunities for more meaningful interactions may be encouraged through longer stays at a destination or choosing to partake in shared or local rituals over superficial sightseeing (Soulard et al., 2021). Encounters with other cultures and perspectives may further evoke empathy and a deeper, more nuanced worldview (Pung & Chiappa, 2020). Certain travel styles, including backpacking, voluntourism, and wellness tourism, are often associated with greater transformative potential due to their immersive and reflective nature.
Wellbeing tourism
Wellbeing tourism is defined as travel “aiming to promote and maintain the health of the body, mind, and soul, while striving for a continuous state of balance and harmony” (Hjalager & Flagestad, 2012). It is closely related to wellness tourism but is distinguished primarily through its association with Nordic countries . While these terms may thus be used interchangeably, a few key distinctions, mainly regional and cultural, should be noted.
In addition to unique geographical features such as fjords, boreal forests, and Arctic tundra, Nordic countries are celebrated for their clean air and water, vast pristine landscapes, and exceptional qualities of light—elements that provide an ideal backdrop for interactions with nature, which are integral to Nordic culture (Hjalager & Flagestad, 2012). Moreover, there is a traditional recognition that personal well-being is inextricably linked to the well-being of the surrounding environment (Hjalager & Flagestad, 2012). This is reflected in wellbeing tourism activities that involve both sustainable and harmonious interactions with nature, as well as meaningful and respectful connections with local communities.
Given these long-standing traditions, while both wellness tourism and wellbeing tourism typically take place in natural environments, the latter is not only associated with stays at wellness resorts but also encompasses a variety of settings, such as eco-retreats, farm stays, rustic camping, and cultural immersion experiences. Wellbeing tourism also includes activities that focus on sustained efforts at holistic well-being. These activities emphasize non-material aspects of well-being, such as escaping routines and achieving mental tranquility, to provide a deeper sense of fulfillment and purpose (Hjalager & Flagestad, 2012). By contrast, wellness tourism typically centers around personal development and transformation, with a greater emphasis on luxury accommodations, pampering, and the consumption of wellness treatments and services.
Yoga Tourism
Yoga tourism is defined as travel for “the express purpose of engaging in yoga practice or where tourists travel with the intention of engaging in yoga practice as a central theme of their trip” (Bowers & Cheer, 2017, p. 211). Yoga tourism is associated with dedicated yoga retreats, seminars, and conferences (Lehto et al., 2006), as well as the growing popularity of outdoor yoga sessions offered over weekends and short breaks, at yoga festivals and in seasonal programs (Grand View Research, 2022).
While some yoga tourists are interested in a fun-filled getaway—often combining yoga with activities like a beach vacation—busy professionals tend to view yoga holidays as a personal luxury and a means of restoring inner harmony and balance, while more dedicated practitioners seek an authentic yoga experience and may travel as far as India to find it (Lehto et al., 2006). India, the birthplace of yoga, has positioned itself as a destination offering authenticity distinct from Westernized yoga practices, accordingly (Bowers & Cheer, 2017).
This distinction rests on the understanding that yoga is, at its core, a spiritual practice; in the West, however, it is often centered on a physical practice and personal development (Lehto et al., 2006, p. 33). Some have labeled the pursuit of personal gain over spiritual growth as “spiritual materialism,” while critics further contend that the commercialization of yoga, especially through tourism, contradicts its historical emphasis on and accessibility as the high costs associated with many retreats may create financial barriers for many (Bowers & Cheer, 2017). Still others have questioned whether yoga tourism aligns with its spiritual origins, arguing that it represents a form of escapism or a refuge from the anxieties of the “real world” rather than a spiritual practice (Bowers & Cheer, 2017).
Despite such criticisms, the numerous benefits of practicing yoga (Dillette et al., 2018) including reported experiences of ‘deep’ transformation, along with the added joy of practicing with like-minded people through yoga tourism, continue to fuel its growth (Lehto et al., 2006, p. 33). In 2021, the global yoga tourism market was valued at $154.11 billion, and it is projected to grow at an annual rate of 5.8% between 2022 and 2030 (Grand View Research, 2022).
History of Wellness resorts and retreats in the United States
Wellness resorts within the United States evolved as a uniquely American product. Their direct predecessors emerged throughout the US for various reasons, rooted in different traditions and have gone as many names, including resort spas, destination spas, sanatariums, health resorts, health farms, health camps, wellness retreats, fitness resorts, and lifestyle resorts.
Toward the end of the 20th century, Stein et al. (1990) identified three main product categories for destination spas based on program emphasis: (1) beauty, (2) fitness and recreation, and (3) spiritual.
In the following sections, we will trace the early history of wellness resorts, beginning with European-style spas. We will also consider the influence of early 20th-century beauty salons, fitness and recreation resorts, and spiritual retreats as well as the emergence of health resorts in the early 1900s. It should be noted that while examples of these early iterations remain, and contemporary wellness resorts still vary in terms of their service offerings and program types, the overall emphasis has converged towards a focus on holistic well-being, in line with contemporary definitions of wellness.
European Spas
The word ‘spa’ is thought to be derived from the old Walloon word espa, meaning fountain, after which the Belgian town of Spa was named. Alternative theories suggest Latin origins, from the word spagere, meaning to scatter, sprinkle, or moisten; from the term sparsa fontana, meaning gushing fountain; or even as an acronym for sanitas per aquas, meaning ‘health through water.’ Regardless of whether the term is of Walloon or Latin origin, the influence of the Roman Empire in establishing spa culture, as well as the popularity of the town of Spa as a health resort in the 16th and 17th centuries, which no doubt solidified its associations, are both rightly acknowledged in its contemporary use.
Spa culture predates the Roman Empire, with ancient civilizations from Greece to Egypt revering thermal and mineral springs (see below) for their healing powers. These springs were often linked to creation myths, water deities, purification rites, and spiritual rituals (Erfurt-Cooper & Cooper, 2009). Archaeological evidence indicates that Paleolithic hunters and Celtic tribes used natural springs as far back as 7000 years ago (Petropoulos, 2014). Bronze Age communities near modern-day Saint Moritz, Switzerland, bathed in iron-rich springs, and artifacts from thermal sites in France and Germany suggest widespread health pilgrimages (Subbaraman et al., 2021).
Pilgrimages to these springs served both religious and therapeutic purposes. Around 4000 BCE, the Sumerians built the earliest known hot spring complexes, featuring elevated temples and flowing pools (Olta et al., 2023). Similar centers emerged in Bronze Age Greece, where natural springs were dedicated to gods (Petropoulos, 2014; Erfurt-Cooper & Cooper, 2009). Notable sites included the sanctuary of Zeus at Olympia and the spa complex at Delphi (Subbaraman et al., 2021). The most famous was the temple of Asclepios, God of medicine and healing, which featured mineral springs, dream temples, and exercise facilities. Patients were treated by priests and attendants until the 4th century CE, when medical care became more secular (Subbaraman et al., 2021). Hippocrates (460–370 BCE), the influential Greek physician who helped secularize medicine, also championed bathing—though as part of a holistic approach to health and healing rather than religious ritual (Van Tubergen & Linden, 2002).
The Romans were heavily influenced by Greek culture and played a pivotal role in establishing and disseminating bathing culture throughout Europe. Like the Greeks before them, Romans recognized the therapeutic properties of mineral-rich and thermal waters, incorporating natural springs, which they termed aquae, into their medical practices. Renowned physicians such as Celsus and Pliny the Elder extolled the virtues of specific springs for their efficacy in treating various ailments. For example, natural springs were used to treat wounds, alleviate rheumatic conditions, and address urogenital diseases. Later, during the Roman Empire, pilgrims, diplomats, and royalty visited the Mediterranean for medical advice and treatment (Subbaraman et al., 2021).
The Romans also constructed sophisticated bath complexes, incorporating various temperatures and types of water for therapeutic and relaxation purposes. Roman baths, known as thermae, were built in population centers and often included spaces for exercise, dining, games, and even libraries and museums. Unlike the Greeks, the Romans placed particular value on the social aspects of bathing, thus laying the groundwork for later European spa traditions. Public baths were accessible to a diverse range of social classes, including the poor, slaves, and women, making them integral to the fabric of Roman society.
Roman bathing culture, however, gradually transitioned towards a greater emphasis on pleasure and indulgence, particularly in the later years of the Roman Empire. Opulent bath complexes became associated with unrestrained excesses and sexual promiscuity. The scandalous behaviors became so pronounced that the word bagnio (from the Italian bango, meaning bathhouse) became a synonym for brothel (Routh et al., 1996). As bathhouses became targets of moral condemnation, they ultimately fell into disuse and disrepair in the closing decades of the Roman Empire.
The Roman military also played a crucial role in establishing spa culture throughout Europe. Spas built around natural springs emerged near military outposts, providing essential facilities for the recuperation of wounded soldiers and offering rest and recreation for healthy troops throughout the territories they conquered. Renowned for their engineering prowess, Roman legions constructed elaborate bath complexes, complete with enclosed pools, steam rooms, and exercise facilities. The presence of these baths would serve as a catalyst for the later development of spa resorts in the same locations. The Roman army’s focus on the medicinal and restorative benefits of bathing also solidified the connection between natural springs, healing, and overall well-being.
With the fall of the Roman Empire, public bathing declined across Europe with the notable exception of Arabic hammams that were established in the 10th–12th centuries in Moorish-controlled Iberia. Such traditional hammam remains popular in parts of Spain today.
Up until the end of the 14th century, widespread opposition to public baths prevailed across much of Europe due to moral and health concerns. In 1350, for example, numerous spas faced destruction following the outbreak of the bubonic plague, fueled by the suspicion that they played a role in its transmission. The fear was not unfounded, as public bathhouses of the time were often crowded spaces where people bathed in the same water for extended periods. This practice contrasted sharply with the stricter bathing practices of earlier periods, particularly those of the Romans, who valued hygiene and recognized the importance of clean water (Routh et al., 1996).
During the Renaissance, the rediscovery of classical texts revived interest in spa treatments among the elite. Spa towns proliferated, and “taking the waters” became a fashionable pursuit. Medical students studied the health benefits of springs, and the chronically ill were prescribed spa treatments while resorts often included medically trained staff and medical services. (Mihalache, 2018).
In traditional European style spas…there may be an ambience redolent of a sanatorium or medical facility, with white decor, or alternatively a luxurious setting reminiscent of the iconic spas of the nineteenth century, with columns or statues (Voigt & Pforr, 2013).
Earlier discoveries of thermal springs in locations destined to become famous spa towns—such as Budapest in Hungary, and Carlsbad (Karlovy Vary) in the Czech Republic—also signaled this future revival. A particularly noteworthy discovery was made in 1326 by Collin le Loup, an iron master from Liège, Belgium, who found chalybeate (iron-bearing) springs in the town that would become known as Spa.
Like other resort towns, Spa’s popularity increased significantly in the 18th century when visiting such places for medicinal purposes became common practice. Spa became especially renowned as a fashionable destination for European aristocracy after Tsar Peter the Great “took the waters” there in 1717. During this time, Spa nicknamed the “Café of Europe,” became synonymous with bathing culture and fitness centers. Baden-Baden, another popular spa town in Germany was likewise the place to see and be seen and was labelled “the most glamorous resort in continental Europe” (Okumus and Kelly, 2023).
Spa culture continued to flourish through the end of the 18th century as a fashionable pursuit for the wealthy, particularly in England and Central Europe, as spas became centers not just for treatment or rest and recuperation, but for social gatherings, entertainment, and cultural activities (Okumus and Kelly, 2023).
In the 19th century, the development of new therapies, such as Kneipp therapy, and the growing accessibility of spas to a wider range of social classes contributed to their continued evolution. Advancements in medical understanding for the time, including analysis of mineral waters, further bolstered the popularity of spas’ therapeutic benefits.
In the early 20th century, European spa culture faltered as a result of the two World Wars, while the rise of modern medicine in their aftermath led to a decline in popularity and government support. Most state-funded visits were cut in Europe, requiring individuals to cover their own expenses for spa visits, which further contributed to the decline in spa attendance.
The latter part of the 20th century, however, witnessed a resurgence as spas adapted to changing social trends. An emphasis on rehabilitation from injury and the curative effects of bathing was largely replaced by a focus on relaxation and preventive healthcare. Erfurt-Cooper and Cooper (2009) further note that, in a marked departure from spas’ original medical focus, the addition of pampering services became a post-World War II phenomenon. Nonetheless, the strong cultural association of spas with the use of natural hot and mineral springs remains a key feature of wellness destinations in Europe, while balneotherapy, the prevention and treatment of disease through bathing, remains fundamental to the wellness concept in a European context. After a period of relative dormancy, Spa tourism in Europe has also more recently reclaimed its position as one of the most important drivers of wellness tourism (Urh, 2015).
American Spas
Today, many types of spas proliferate across the United States, often lacking any connection to their European origins or even a consistent definition. As noted by Stein et al. (1990), “many are unique, a situation that makes it difficult to develop any classification of this industry. In fact, it is challenging to develop a firm definition of what a spa is. A spa can be anything from a hot tub with mineral water to an exclusive, posh resort with body treatments and specialized food service” (p. 46).
At first, however, spas mirrored European traditions, with American bathhouses being built around thermal and mineral springs found throughout the continent (Sigert, 1942). By the early 20th century, no fewer than 2,717 locations with a total of 8,826 mineral or thermal springs had been identified; of these, 424 were commercially managed, with 321 developed as health resorts (Sigert, 1942).
Long before European settlers arrived, Native American tribes had incorporated natural springs into their healing practices and spiritual beliefs (Lund, 1996). Thermal and mineral springs were revered as manifestations of the “Great Spirit,” and their healing powers were interwoven with myths and origin stories (Lund, 1996). These springs also served as neutral gathering places, fostering peace and shared experiences among different tribes (Lund, 1996). While Native Americans often alerted colonialists to the location of such springs (Scribner, 2016), they took their cue for their use and development of from European traditions of “taking the waters” (Spivack, 1997).
Initially, American spas lacked the grandeur of their European counterparts as early colonialists built rudimentary bathing houses until the opening decades of the 19th century after which time resort towns with grand hotels and amenities had begun to flourish (Spivack, 1997). The first bathhouse in Hot Springs, Arkansas, consisted of a single wooden tub, until federal bathhouses were established there in 1878. Dubbed “America’s First Resort,” the Homestead in Virginia’s Allegheny Mountains was founded with the construction of a simple tavern in 1766 (Kelley, 2023). Inspired by European hydrotherapy, Dr. Thomas Goode later opened a medicinal spa there in 1832, which remains in operation today (Kelley, 2023).
In the middle of the 19th century the American spas had a period of great vogue. They were famous, not so much for their waters, as for their horse-races, gambling places, theaters, and other entertainments. They were resorts of the idle and rich, with luxurious hotels, parks and casinos. The waters were used, to be sure, because it was fashionable to use them, but in most cases they were a mere accessory and a pretext for social life (Sigerist, 1942).
Like their European counterparts, American spas served diverse purposes, from therapeutic and restorative to social and recreational, and the guests who frequented them ranged from the seriously ill to those seeking pleasure and high society (Sterngass, 2001). Those individuals who visited natural mineral springs for their healing properties often followed specific regimens under medical supervision, as the waters were administered for ailments ranging including diabetes, diarrhea, and night sweats (Shelton et al., 1923).
Such spas also provided a scenic escape from daily life, offering relaxation and rejuvenation in nature. Some sites, for example, became fashionable summer retreats for Southerners seeking an escape from the risk of contracting malaria and the oppressive seasonal heat. For women in particular a stay at a spa that entailed daily bathing, lighter clothing, and relaxed etiquette, represented a rare liberation from the social constraints of the period (Sterngass, 2001). Spa resorts were also social hubs where the wealthy mingled and leisure activities like dances, performances, and other entertainment took place alongside health pursuits. By the 1830s, the “Springs Tour” was fashionable among the social elite, which involved visits to multiple spring resorts in succession.
The most famous spa resorts would come to rival their European counterparts in terms of the medical regimes, infrastructure, and social and cultural pursuits. Saratoga Springs, New York, first introduced to European settlers by the Mohawk Indians, was visited by George Washington in 1783. The first tavern was constructed there in 1803, and a growing settlement was incorporated as a separate township in 1819. At its height, Saratoga Springs was a fashionable resort that drew thousands of visitors from various social classes who came for the mineral waters, social life and entertainment including horse races, gambling, and theaters. Once boasting opulent Greek Revival hotels that could accommodate up to 500 guest, Saratoga Springs gained a reputation as the “Baden-Baden of America” (Weiss, 2004).
By the late 19th century, however, spa resorts had begun to decline. The Civil War disrupted the southern clientele who had bolstered popular resorts such as Saratoga Springs and in the wars aftermath, changing fashions and fortunes permanently altered these travel patterns. Medical advancements in antibiotics and vaccines had also reduced the perceived need for hydrotherapy. While some spas incorporated golf courses and other new forms of entertainment to attract tourists, most fell into disuse. The rise of alternative fashionable destinations, such as seaside resorts, further contributed to spas’ decline.
The two World Wars and the interim Great Depression signaled the death knell for spa culture as changing social attitudes and economic constraints made spa visits less feasible. Scientific advances in the 20th century and the rise of conventional medicine further marginalized hydrotherapy which had come to be seen as unscientific and ineffective. Whereas European spas retained their association with medical and health-based therapies, American spas took on a different role as spaces focused on beauty and relaxation rather than therapeutic treatments. Although a small revival occurred in the latter part of 20th century, such resorts never regained their former prominence and today, the word spa itself is far more likely to evoke images of facials, pedicures, massages, and luxury products in aesthetic environments than natural springs (Little, 2013).
Thalassotherapy
Thalassotherapy refers to medically supervised seawater treatments most common in France, Ireland, and Spain (Spa Index, 2006). The term (from the Greek thalasso meaning sea, and therapeia meaning treatment) was coined in France in 1867 where the use of seawater and marine plants for health and beauty was first pioneered (Kelly, 2024). According to the International Federation of Thalassotherapy, related practices involve the medically supervised use of the marine environment for preventive or curative purposes (Kelly, 2024).
Although the U.S. has yet to fully embrace thalassotherapy, the seaside has been popular for both recreational and wellness purposes since the mid-19th century. Prior to that, oceans and shorelines were often viewed as foreboding, ominous places; it wasn’t until Romantic artists and poets re-imagined them as sublime settings conducive to revitalization and introspection that they began to capture the public imagination (Aron, 1999).
As public perceptions changed and coastlines became more accessible through rail and automobile travel, seaside resorts began to flourish. Established in the late 1800s, Atlantic City was America’s first resort city, attracting large numbers of both middle and upper-class visitors (Miller, 2008). Offering plenty of sea, sun, sand, and fresh air along with recreational and social opportunities, seaside resorts soon surpassed the popularity of the more traditional spa towns (Mill, 2008). Although the therapeutic value of marine environments and their by-products has more recently gained appreciation (Aron, 1999), Gurney’s Montauk Resort and Seawater Spa is the only spa in the U.S. that currently offers a range of traditional thalassotherapy services (Kelly, 2024).
Cosmetic: beauty salons
The early 20th century saw the rise of beauty salons and luxury spas, of which Elizabeth Arden’s iconic Red Door Salon is the most famous example. Arden, born Florence Nightingale Graham to English and Scottish parents in Ontario, Canada, emigrated to New York City in 1908. In 1909, Graham bought the Elizabeth Hubbard beauty shop on Manhattan’s Fifth Avenue, where she and then proprietor Hubbard planned to enter into business together (Nelson, 2015). Their partnership soon floundered, however, but as the name “Elizabeth” had already been inscribed on the salon’s door at some expense, Graham decided to keep it, adding the name “Arden” from the title of her favorite Tennyson poem, Enoch Arden. She would use this as her business name for the rest of her life (Nelson, 2015).
Growth in women’s fitness in the early 20th century came not from federal investment or from athletics. Rather, tending to the body for beauty became a powerful way that a nascent industry sold figure control and slenderizing at first through passive exercise to women…with new products and spaces such as slenderizing spas that employed gentle exercise to help women reduce in luxurious comfort without disrupting any notions of conventional femininity and certainly without compelling women to enter gymnasiums which were off-puttingly public and often overwhelmingly male spaces (Petrzela, 2023).
Catering to a more affluent segment of New York society, an extended visit to Arden’s Red Door Salon might include a combination of steam room, massage, manicure, pedicure, facial, hairstyle, and make-up, combined with an exercise class and a light, healthful lunch (Nelson, 2015). The class would have focused on rhythmic, lady-like movements or employed fitness machines that allowed women to exert minimal effort while their bodies were put through an ‘exercise’ routine (Petrzela, 2023). Such studios equipped with posture correction and stretching machines, wall-mounted pulleys for light toning, or other passive beauty enhancements were frequently located within or alongside beauty salons as gymnasiums were coarse, male-dominated domains entirely unsuited to genteel patronage.
The first destination spa was also the brainchild of Elizabeth Arden, who opened Maine Chance Farm in Mount Vernon, Maine, in 1934. Maine Chance offered a variety of spa and beauty treatments, light meals, and moderate exercise, essentially replicating the services and treatments offered at her salons, albeit with overnight stays.
In 1945, Elizabeth Arden opened a second Maine Chance luxury spa in Phoenix, Arizona. Catering exclusively to women, it promoted the idea that timeless beauty could be maintained through proper diet, exercise, and spa treatments (Stein et al., 1990). The spa offered an à la carte menu alongside a restricted 950-calorie-a-day weight loss program, as well as fitness classes, tennis, and pool workouts. This reflected the post–World War II shift in attitudes, as more strenuous exercise had become acceptable for women (Petrzela, 2023; Stein et al., 1990). Spa amenities included whirlpools, saunas, steam rooms, and facilities for facials, massages, and other treatments. Educational classes on makeup, skincare, and healthy cooking were also offered (Stein et al., 1990).
Both Maine Chance spas eventually fell out of step with the times. The Mount Vernon location closed for good in 1970 following a fire, while the Arizona property was sold and incorporated into an all-inclusive holiday resort. However, other luxury spas catering to an affluent, mostly female clientele emerged—most notably the legendary Golden Door Spa in California. Established in 1958 as a sister site to Rancho La Puerta (see below), it is still in operation today. By the end of the 20th century, luxury spas offering top-tier services and amenities, combined with a great deal of pampering, represented roughly 8% of destination spas nationwide (Spivack, 1998).
milk farms
A 1938 Life Magazine article entitled, They Lose a Pound a Day the Milk Farm Way, highlighted the popularity of so-called milks farms. As a contemporary counterpart to the ‘health farm’ which catered to male, urban office workers in the habit of “slipping off for a couple of weeks of clean living and hard exercise”, milk farms targeted “stylish stouts” wanting to shed pounds from their “oversize figures” (Life, 1938, p.36).
Rose Dor Farm in New York was a prime example. Described as a swank country club, the farm’s weight loss regime required a minimum ten day stay that included a “strict diet” consisting of three days of fruit and vegetable juices followed by seven days of cultured milk and vegetables, along with daily does of “scientific exercise” (Life, 1938).
At a time when lady-like behavior was still at odds with physical activity, these scientific exercise routines amounted to women, clad in shorts, make-up and heels, doing mat stretches or receiving “passive manipulation” of their limbs by the exercise instructor; in fact the only good sweat these women appeared to achieve was after being rubbed down and swaddled in hot blankets, a body treatment offered as part of the program and referred to as a herbal massage (Life, 1938, p.37).
Health Resorts
Early health resorts were established as both alternative centers for treating chronic conditions such as tuberculosis as well as health-conscious individuals who sought rest and rejuvenation in restorative environments. Sanitariums first appeared in the 1800s. While the term later acquired negative connotations, the word, rooted in sanitary, simply reflected the era’s preoccupation with dirt and disease, or more precisely, their eradication rather than confinement for mental disorders (Tackett, 1990).
A notable example was the Battle Creek Sanitarium, established by Seventh Day Adventists in Michigan in 1866. In 1876, Dr. John Harvey Kellogg, of box cereal fame, was appointed Chief Physician and played a pivotal role in Battle Creek’s development. No medications were administered. Rather, Kellogg, a firm believer in the healing powers of sunshine, often prescribed sunbaths for his patients. He also introduced alternative treatments such as hydrotherapy and electrotherapy and conducted research on nutrition and exercise.
A stay at the sanitarium consisted of a strict regimen of two meals per day served five hours apart. Along with meatless diets, for which purpose the grounds were equipped with a dairy farm and several fruit and vegetable gardens, abstinence from alcohol and tobacco was enforced. Morning and evening exercises were prescribed for all those physically able, while patients wore loose fitting clothing, freeing women from constricting corsets. In addition to a large gymnasium equipped with various apparatus, Swedish movement or exercise machinery that mechanically massaged the body and treated various muscular groups, calisthenics, swimming, and outdoor activities were commonplace.
Under Kellogg’s leadership, the sanitarium expanded its facilities and became a world-renowned institution celebrated for its innovative treatments. Battle Creek was also described as a vibrant and popular place that offered a restorative and healing environment, attracting many including both prominent Americans and international visitors (Tackett, 1990). A casualty of the Great Depression, however, Battle Creek closed its doors for good in 1937.
Other health resorts of the late 1800s offered opportunities for recuperation, rest, and rejuvenation, as well as for a new kind of malady that was on the rise, dubbed Americanitis (Tackett, 1990). This referred to nervous disorders attributed to the harsh working conditions and societal upheaval wrought by the Industrial Revolution. The remedy, leisure holidays, was often prescribed by doctors who encouraged their patients to seek restorative environments such as mountains, deserts, and coastal areas in what was collectively termed “climatic therapy” (Tackett, 1990).
The southwestern US was replete with conducive environments, and independent of the European-style spa culture that had developed on the East Coast, health tourism formed around local natural resources. Prior to 1900, an estimated 25 percent of the total influx of people arriving in Southern California were seeking cures for ailments, most commonly tuberculosis (Culver, 2010). Similarly, the first “tourists” to the Coachella Valley were seeking relief from various afflictions (Culver, 2010). To take advantage of this travel market, the Southern Pacific railroad company constructed a number of holiday cottages for “consumptives” along its westward route, while the Palm Springs Hotel in Indio, CA, built by the self-described “Dr.” Welwood Murray in 1888, gave guests easy access to local hot springs (Culver, 2010). In the mid-1900s, an investor well aware of the potential for the development of Catalina Island, just off the coast of what is today Los Angeles, noted: “Of greatest importance…is the sustainability of this island as a health resort and the consequent influx of population and settlers. A sanitarium…would never cease to attract those desiring outdoor life in continual sunshine, an equitable temperature with gentle but exhilarating sea breezes, freedom from the vexations of more crowded resorts, and escape from the ravages of consumption, rheumatism, and malaria” (Culver, 2010, p. 96).
Beginning in the 1900s, tourists also wintered in the Scottsdale, Arizona desert. Visitors came at the recommendation of their doctors to recover from lung conditions and arthritis, while others came simply to “relax, rejuvenate, reduce, and reclaim health and wellbeing” (Fudala, 2022). Some health camps also incorporated Native American wisdom, particularly that of the Salt River Pima-Maricopa Indian Community, whose understanding of the benefits derived from desert plants such as aloe and jojoba were used as natural remedies and treatments (Fudala, 2022).
Guest ranches
In the 1800s, industrialization prompted many Americans to seek outdoor leisure activities. A growing tourist economy focused on experiences in nature also coincided with the westward expansion of the railroad (Coleman, 2011). During this time, dude ranches emerged—recreational guest ranches that offered visitors the opportunity to experience the lifestyle of a working ranch, with activities such as horseback riding, fishing, hiking, and nature walks (Coleman, 2011). Despite prevailing gender norms, many women also participated in these outdoor pursuits from the late 1800s onward (Coleman, 2011).
Other ranches, particularly in the Southwest, positioned themselves as places for rest and rejuvenation, along with the health benefits of a warm, dry climate. Graves Guest Ranch in Scottsdale, Arizona, was one of the earliest of these ranch style health camps, operating from the early 1900s through the 1950s (Fudala, 2022). While accommodations consisted of rustic tent cabins, guests at Graves were provided with “home cooked meals of local farm produced fruit, citrus, vegetables, dairy, and meat; and gentle outdoor activities that included croquet, riding horses, and hiking to picnics” (Fudala, 2022).
By the mid nineteenth century, professional outdoor guides were offering social elites and a growing number of industrial workers authentic Western experiences. The rising popularity of the automobile in the early 1900s further supported the spread of outfitters, hunting and fishing lodges, mountaineering clubs, and dude ranches. By 1925, as many as 350 dude ranches were in operation (Coleman, 2011). Today, a number of dude ranches remain, some of which have diversified to offer spas treatments, reflecting both their own evolution and the broader influence of wellness on the tourism and hospitality industry.
Fitness And recreation
The first example of a modern wellness resort as we know them today is Rancho La Puerta (see below). Established in Tecate Mexico in 1940, it evolved into a model for many of the wellness resorts that followed, especially given the resounding success of its programs and ethos (Spivack, 1997). At the time, however, Rancho La Puerta was very much the exception. Both the Great Depression and World War II stunted wellness travel in the first part of the 20th century as most Americans had neither the means nor inclination for leisurely holidays (Stein, 1990). Medical advances and changing views in the 1940s and 1950s had also eroded support for alternative therapies such as hydrotherapy (Spivack, 1998).
Societal shifts in the 1960s created new momentum for wellness vacations, the rise of which paralleled the “fitness craze” of the coming decades (Klemesrud, 1972; Stein et al., 1990). Related countercultural influences and changing social norms further encouraged holistic practices reflective of overall trends towards personal well-being and longevity (Spivack, 1997). A growing number of Americans, most of them white and affluent, spurred by the health foods craze, the youthquake, more leisure time and the “slim is‐in” fashion philosophy….decided to combine their sun‐and‐surf sojourns with shape‐up programs designed to make them look, and feel, better (Klemesrud, 1972).
The resort industry’s response to popular demand resulted in dozens of new health resorts being built especially in warm weather states (Klemesrud, 1972). Between 1978 and 1994, the number increased from 50 to 300, and by 1990, more than 5 million Americans were spending their vacation time at health resorts across the nation (Tackett, 1990; Spivack, 1997). Canyon Ranch, opened in 1979, is one such example. Located in an ideal spot for hiking and relaxation amid the beautiful mountains and desert landscapes of Tucson, AZ Canyon Ranch offered a program that promoted improved overall well-being through good living (Spivack, 1998). Canyon Ranch has since expanded to include resorts and wellness clubs in locations such as Lenox, Woodside, Las Vegas, and Fort Worth and offers all-inclusive wellness stays, spa services, and curated experiences.
Not all programs established in the 1970s had lasting appeal. Many resorts came to earn pejorative labels like “fat farms” or “fat camps” as their programs focused primarily on weight loss through Spartan diets and rigorous exercise regimens (Alpern, 1977). Some of these resorts straddled the line between preventive and curative programs, addressing chronic conditions such as high blood pressure, angina, and heart disease associated with obesity. In certain cases, the costs of stays were even eligible for coverage by health insurance plans (Spivack, 1997). However, the extreme methods employed, including drastic calorie restrictions and, in many cases, militant physical instruction, were later recognized as unsustainable and potentially harmful (Risius, n.d.).
By the late 1980s, such health resorts had rebranded as fitness retreats or lifestyle resorts, emphasizing lifestyle changes through enjoyable exercise routines and nutritious meals (Calistro, 1987; Franckling, 1988). Shedding negative associations with “fat farms” a common goal was to equip participants with diet and exercise plans, along with behavior modification and stress relief strategies to promote long-term well-being beyond the stay itself (Calistro, 1987). Cross training emerged as a popular method for achieving full body fitness, with the potential for guests to incorporate some of the activities into their daily lives (Calistro, 1987). These resorts also prided themselves on improving guests’ mental health by encouraging work life balance and coping mechanisms, as well as offering behavior modification, nutrition advice, and counseling (Calistro, 1987). Others replaced the luxuries of early destination spas with a more clinical approach; for example, guests might hike seven miles under the guidance of a kinesiologist or exercise on a treadmill monitored by a nurse (Calistro, 1987). Thus, many resorts came to align with more contemporary attitudes toward holistic well-being and programs now typical at wellness resorts.
Highlight: Rancho La Peurta
Rancho La Puerta, simply called “The Ranch,” is located in Tecate, Baja California, 45 miles southeast of San Diego, near the U.S.-Mexico border. Founded in 1940 by Edmond and Deborah Szekely, it has evolved into one of North America’s most renowned wellness resorts. As the first fitness-oriented destination spa, it drew inspiration from the Essenes, an ancient Jewish sect that emphasized simplicity, connection with nature, and holistic living. The Szekelys aimed to recreate the Essenes’ cooperative lifestyle, encouraging guests to engage in gardening and food preparation while focusing on natural healing methods like a vegetarian diet, fresh air, and exercise. In addition to its Essene inspiration, Rancho La Puerta embraced elements from ancient Mexican cultures, especially in its architecture, landscaping, and activities. Professor Szekely, captivated by these ancient traditions, integrated them to craft an authentic and immersive experience for guests.
Initially, Rancho La Puerta operated as a rustic summer camp, where the founders introduced herbal wraps to help guests recover from sore muscles after hiking and activities. Over the years, the Szekelys expanded offerings by enlisting experts to create massage and skincare training programs, enhancing the guest experience. While massages were initially intended to soothe post-exercise soreness, the ranch emphasized a philosophy of “fitness of body and mind.”
Today, Rancho La Puerta blends its historical focus on fitness and simple living with modern wellness experiences. It offers over 70 indoor and outdoor fitness classes each week, including yoga, Pilates, and hiking. The spa features a wide range of treatments, including various massages, body wraps, and facials. Accommodations include 87 private rooms and luxury Villas Cielo, each designed for comfort and relaxation. Culinary offerings highlight semi-vegetarian cuisine with organic ingredients, and guests can participate in cooking classes at “La Cocina Que Canta.” The ranch also provides diverse afternoon and evening programs, from lectures to arts and crafts. Other amenities include multiple gyms, swimming pools, tennis courts, and a meditative labyrinth.
Spiritual: retreats and ashrams
The term retreat may refer either to a physical center or a curated, multi day wellness program as described in Chapter 5: The Wellness Industry. In this section, the terms refers to places dedicated to “quiet reflection and rejuvenation, an opportunity to regain good health, and/or…a time for spiritual reassessment and renewal, either alone, in silence, or in a group” (Kelly, 2010, p. 109).
At St. Mary-by-the-Sea….the centuries-old practice of traveling to a secluded spot for an intense period of silent renewal and reflection, is no longer the province solely of avowed Catholic sisters. Decades of decline in the number of women taking religious vows, juxtaposed with an increase in people describing themselves as spiritual but not religious, has created a sea change, if you will, in attendance at retreats. Group and individualized retreats are increasingly popular among the Christian laity…for whom spirituality has supplanted religion (Marder, 2009). Retreat centers have roots in religious and spiritual traditions the world over (Cloutier, 2015). In the West, they began with Catholic monasticism, where monks withdrew for spiritual reflection, a practice later extended to pilgrims and laypeople through monastery stays, still popular in Europe and the U.S. In the late nineteenth century, American Protestants held retreats in the form of summer camps at Chautauqua Lake, New York, blending religious teachings with cultural, educational, and self improvement programs (Aron, 1999). These camps expanded via traveling circuits and permanent resort centers established in other locations. Though their popularity waned by the 1930s, the Chautauqua Institution continues to offer retreats today.
Ashrams originated in ancient India as hermitages where sages lived and meditated far removed from worldly distractions, but these evolved into structured centers which have attracted visitors for millennia and are now also found elsewhere. The first ashram community in the United States was established in the early twentieth century and their subsequent growth in numbers reflected the interest in Eastern spirituality that surged in the US in the post World War II era, particularly during the 1960s. The Ananda Ashram in Rhinebeck, New York, for example, was founded in 1964 by Swami Kriyananda to teach Indian spiritual practices.
Although some include a spiritual focus such as Hindu ashrams and Buddhist meditation centers (see below), wellness retreats, also referred to as New Age retreats, are typically non denominational (Spivack, 1998), preserving a link to traditional religious retreats through an emphasis on seclusion. Breitenbush Hot Springs in Detroit, Oregon, for example, describes itself as a sanctuary offering personal retreats for healing, relaxation, and connection with nature. Other wellness retreat centers reflect a holistic approach, including mind body programs and alternative therapies (Spivack, 1998). The Art of Living Retreat Center in Boone, NC, for example, offers yoga, meditation, and other healing practices rooted in ayurvedic principles.
Retreat centers are often found in unique or remote locations to help participants disconnect from their daily routines and immerse themselves in the natural world and/or inner reflection (Trimble, 2024). Unlike other styles of wellness resorts, they also typically do not offer extensive pampering or spas services, and accommodations may be spartan, as personal development is prioritized over material comforts (Spivack, 1998). This is also reflected in the price of stays, which tend to be lower than the average wellness resorts. Omega Institute in Rhinebeck, New York, for example, provides a variety of wellness and mindfulness programs and is a popular and affordable option for those seeking holistic well being . New Age retreats represented an estimated 18 percent of all destination spas in the US by the end of the twentieth century (Spivack, 1998).
Buddhist Retreat Centers
A number of retreat centers in the US are hosted by Buddhist communities. The Insight Retreat Center in Santa Cruz, CA, for example, offers opportunities to engage in spiritual practices and and inner reflection. The facility offers residential retreats that accommodate around 30 participants and their popularity is evidenced by the fact that spots fill around three months in advance (Norman & Pokorny, 2017). Retreat programs include structured group meditation, lectures, and individual practice, typically lasting from a single night to several days.
Set in the serene environment of the Ozarks, Arkansas, the Katog Rit’hröd mountain retreat center was founded in 2007 and has seen a steady influx of visitors since, with some individuals moving into the centers rudimentary wooden cabins for extended stays. The center typically attracts up to 250 practitioners for two- to eight-week retreats, who are accommodated in the community lodge or camp on the grounds by donation (Weissberg, 2023). The center offers guided programs with spiritual practices aimed at helping individuals cultivate inner peace and understanding through Buddhist teachings.
Which knowledge, skills, and abilities are supported by this chapter?
This chapter integrates an understanding of wellness as the pursuit of holistic well-being with the travel industry’s supply-side dynamics. It emphasizes the distinction between wellness tourism and general travel and leisure pursuits, while also addressing definitional complexities and overlaps with related niche segments such as spa, medical, and spiritual tourism. A historical context deepens appreciation for, and the ability to differentiate among, the diverse types of wellness tourism destinations in operation, destinations that draw from a rich and varied lineage including Euro-inspired hydrotherapy, beauty spas, sanitariums, destination spas, and New Age retreats. This foundation may inform the design and marketing of wellness destinations and experiences that are authentic, culturally attuned, and aligned with a nuanced focus on the physical, emotional, and spiritual dimensions of well-being.
Review Questions
What are some of the challenges associated with defining wellness tourism as a sub-sector?
In what ways has the rise of medical tourism challenged traditional healthcare delivery in both source and destination countries?
Why is the term ‘health tourism’ particularly useful in a European context, and how does this differ from global usage?
Discuss how spiritual tourism reflects broader societal trends toward individualism, personalization, and the search for meaning.
Why is transformative tourism considered more of an approach than a specific type of tourism? Provide examples.
How does wellbeing tourism reflect Nordic cultural values, and how does it differ from wellness tourism in terms of setting and philosophy?
How does yoga tourism exemplify the intersection of spiritual, wellness, and transformative travel motivations?
How did societal attitudes toward women and physical activity influence the development of beauty spas and fitness resorts in the early 20th century?
Analyze how the fitness and lifestyle resorts of the 1970s–1990s transitioned toward holistic wellness models. What broader cultural trends facilitated this shift?
What distinguishes a wellness retreat from a typical wellness resort?
references
Alpern, D. M. (1977, April 10). A Hale at Large In a ‘Fat Farm’. New York Times. https://www.nytimes.com/1977/04/10/archives/a-male-at-large-in-a-fat-farm-a-male-weighs-in-at-a-health-spa.html?auth=login-google1tap&login=google1tap#
Aron, C. S. (1999). Working at play: A history of vacations in the United States. Oxford University Press.
Beebe, A. (1949). The History of Battle Creek Sanitarium. Papers from the History Seminar of Kalamazoo College.
Björk, P., Tuohino, A., & Konu, H. (2011). Wellbeing tourism in Finland-A wide perspective. Matkailututkimus, 7(2), 26-41.
Bodeker, G., & Cohen, M. (Eds.). (2010). Understanding the global spa industry. Routledge.
Bookman, M. Z., & Bookman, K. R. (2007). Introduction to medical tourism. In Medical tourism in developing countries (pp. 1-19). New York: Palgrave Macmillan US.
Borja, M. (2019, July 25). Summer Camp: American Religion and Recreation in the Great Outdoors. Patheos. https://www.patheos.com/blogs/anxiousbench/2019/07/summer-camp-american-religion-and-recreation-in-the-great-outdoors/
Bowers, H., & Cheer, J. M. (2017). Yoga tourism: Commodification and western embracement of eastern spiritual practice. Tourism Management Perspectives, 24, 208-216.
Braçe, O., Garrido-Cumbrera, M., & García-Marín, R. (2023). Approaches to health tourism from the geography. Definition and study field. Cuadernos de Turismo, (51), 429-432.
Calistro, P, (1987, August 9). The Latest Resorts : A New Kind of Spa Forgoes Both Frills and Fat-Farm Rigors in Favor of Fitness Re-Education. Los Angeles Times. Travel and Experiences. https://www.latimes.com/archives/la-xpm-1987-08-09-tm-358-story.html
Carrera, P. M., & Bridges, J. F. (2006). Globalization and healthcare: understanding health and medical tourism. Expert review of pharmacoeconomics & outcomes research, 6(4), 447-454.
Chen, C. C., & Petrick, J. F. (2013). Health and wellness benefits of travel experiences: A literature review. Journal of Travel Research, 52(6), 709-719.
Chen, J. S., Prebensen, N., & Huan, T. C. (2008). Determining the motivation of wellness travelers. Anatolia, 19(1), 103-115.
City of Arkansas. (n.d.) History of Hot Springs. https://www.cityhs.net/DocumentCenter/View/183/History?bidId=
Cohen, M., & Bodeker, G. (Eds.). (2008). Understanding the global spa industry: Spa management. Routledge.
Coleman, A. G. (2011). The Rise of the House of Leisure: Outdoor Guides, Practical Knowledge, and Industrialization. Western Historical Quarterly, 42(4), 436-457.
Collins-Kreiner, N. (2020). Pilgrimage tourism-past, present and future rejuvenation: a perspective article. Tourism review, 75(1), 145-148.
Cooper, W. (n.d.). Medical Tourism: What Is Health Tourism & Where Is It Popular?. https://www.william-russell.com/blog/what-is-medical-tourism/
Cloutier, J. A. (2015). The Significance of Community in Wellness Service Design: The Case of Retreats (Doctoral dissertation, Master’s thesis, University of Tartu, Estonia), http://dspace. ut. ee/bitstream/handle/10062/49423/cloutier_josee-ann. pdf
Culver, Lawrence. The frontier of leisure: Southern California and the shaping of modern America. Oxford University Press, 2010.
Daniel, S., Tomljenović, R., Klarić, V., Pleša, I. Č., & Klarić, J. (2022). EUSAIR Wellbeing Tourism Handbook. Ministry of Tourism and Sport of the Republic of Croatia. Retrieved from https://mint.gov.hr/UserDocsImages/2022_dokumenti/221228_WELLBEING_handbook.pdf
Dhami, N. (2013). Trends in Pharmacognosy: A modern science of natural medicines. Journal of herbal medicine, 3(4), 123-131.
Dillette, Alana K., Alecia C. Douglas, and Carey Andrzejewski. “Yoga tourism–a catalyst for transformation?.” Annals of Leisure Research 22, no. 1 (2019): 22-41.
Dimitrovski, D., & Todorović, A. (2015). Clustering wellness tourists in spa environment. Tourism Management Perspectives, 16, 259-265.
Dulles, F. R. (1940). American Learns to Play: A History of Popular Recreation 1607—1940. D. Appleton-Century Company.
Erfurt-Cooper, P., & Cooper, M. (Eds.). (2009). Health and wellness tourism: Spas and hot springs, 40. Channel View Publications.
European Travel Commission. (2018). European Travel Commission (ETC) and World Tourism Organization (UNWTO) Exploring Health Tourism, Executive Summary. https://etc-corporate.org/uploads/reports/2018-ETC-UNWTO-Exploring-Health-Tourism-Executive-Summary.pdf
Filep, S., & Pearce, P. (Eds.). (2014). Tourist experience and fulfilment. Insights from Positive Psychology. Taylor and Francis.
Franckling, K. (1988, June 3). This spa is no ‘fat farm’. UPI. UPI Archives. https://www.upi.com/Archives/1988/06/13/This-spa-is-no-fat-farm/3145582177600/
Fudala, (2022, January 15). Sunny Scottsdale is A Historic Spa Haven. Insiders Guide to Spas. Spa Culture. https://www.insidersguidetospas.com/features/sunny-scottsdale-is-a-historic-spa-haven/
Georgiev, G. & Vasileva, M. (2010). Some Problems Related to the Definitions of Balneo, Spa and Wellness Tourism. Proceedings of the Biennial International Congress. Tourism & Hospitality Industry; Opatija. 902-909.
Glow MedSpa. (2023, September 8). What is a Medical Spa? Here’s Where Science Meets Beauty. https://www.glowmedspa.com/what-is-a-medical-spa/
Grabar, H, (2015, November 16, 2015). What Became of America’s Water-Cure Towns? Bloomberg. Culture. Retrieved from https://www.bloomberg.com/news/articles/2015-11-16/the-legacy-of-america-s-water-cure-towns
Grainger, B. M. (2019). Church in the wild: evangelicals in antebellum America. Harvard University Press.
Grand View Research. (2022, August). Yoga Tourism Market Size, Share & Trends Analysis Report By Gender (Women, Men), By Region, And Segment Forecasts, 2022 – 2030. https://www.grandviewresearch.com/industry-analysis/yoga-tourism-market-report
Hall, C. M. (Ed.). (2012). Medical tourism. Abingdon: Routledge.
Halim, M. S. A., Tatoglu, E., & Hanefar, S. B. M. (2021). A review of spiritual tourism: A conceptual model for future research. Tourism and hospitality management, 27(1), 119-141.
Hesselberth, P. (2021). Retreat culture and therapeutic disconnection. In Jansson, A., & Adams, P. C. (Eds.) Disentangling: The geographies of digital disconnection, 253.
Hjalager, A. M., & Flagestad, A. (2012). Innovations in well-being tourism in the Nordic countries. Current Issues in Tourism, 15(8), 725-740.
Huang, X., Wang, P., & Wu, L. (2024). Well-being through transformation: An integrative framework of transformative tourism experiences and hedonic versus eudaimonic well-being. Journal of Travel Research, 63(4), 974-994.
Howard, J. & Chavez, J. (2023, March 8). Medical tourism to Mexico is on the rise, but it can come with risks. CNN. Health. https://edition.cnn.com/2023/03/07/health/medical-tourism-mexico-trend-wellness/index.html
Hudson, S., & Li, X. (2012). Domestic Medical Tourism: A Neglected Dimension of Medical Tourism Research. Journal of Hospitality Marketing & Management, 21(3), 227-246.
Kelley, S. (2023, January 24). The Homestead: America’s First Resort – Wanderlust Tours. Wanderlust Tours. https://wanderlust-tours.com/thehomestead/
Kelly, G. (2024, April 30). Thalassotherapy: Beauty from the Sea. Organic Spa Magazine. https://www.organicspamagazine.com/thalassotherapy-beauty-from-the-sea/
Kelly, C., & Smith, M. K. (2016). Journeys of the self: The need to retreat. In The Routledge handbook of health tourism (pp. 166-179). Routledge.
Klemesrud, J. (1972, January 23). Tice Fat Farms—Or, How To Come Home A Real Loser. The New York Times. https://www.nytimes.com/1972/01/23/archives/the-fat-farms-or-how-to-come-home-a-real-loser-the-fat-farm-limit.html
Konu, H., Tuohino, A., & Björk, P. (2011). Wellbeing tourism in Finland: Finland as a competitive wellbeing tourism destination. Nordic Innovation Center. Retrieved from https://erepo.uef.fi/bitstream/handle/123456789/10714/urn_isbn_978-952-61-0585-7.pdf
Kujawa, J. (2017). Spiritual Tourism as a Quest. Tourism Management Perspectives, 24, 193-200.
Large, D. C. (2015). The grand spas of Central Europe: a history of intrigue, politics, art, and healing. Rowman & Littlefield.
Laws, E. (2015). Health Tourism: A business opportunity Approach. In Clift, S. & Page, S. (Eds.). Health and the International Tourist. (2nd ed.). Routledge.
Lehto, X. Y., Brown, S., Chen, Y., & Morrison, A. M. (2006). Yoga tourism as a niche within the wellness tourism market. Tourism Recreation Research, 31(1), 25-35.
Life. (1938, August 15). They Lose a Pound a Day the Milk Farm Way. Modern Living. https://books.google.com/books?id=gE8EAAAAMBAJ&pg=PA36&#v=onepage&q&f=false
Little, J. (2013). Pampering, well-being and women’s bodies in the therapeutic spaces of the spa. Social & Cultural Geography, 14(1), 41-58.
Lund, J. W. (1996). Balneological use of thermal and mineral waters in the USA. Geothermics, 25(1), 103-147.
Lunt, N., & Carrera, P. (2010). Medical tourism: assessing the evidence on treatment abroad. Maturitas, 66(1), 27-32.
Mackintosh, W. (2012). ” Ticketed Through”: The Commodification of Travel in the Nineteenth Century. Journal of the Early Republic, 32(1), 61-89.
Marder, D. (2009, July 29). Sea change in retreats: The spiritual, rather than religious, join nuns at retreat. Philadelphia Inquirer (Philadelphia, PA). Philadelphia Media Network
Medical Tourism Association. (2024). Medical Tourism Unveiled: Why Patients Travel and What Holds Them Back: A Deep Dive into the Medical Tourism Decision-Making Process. https://cdn.prod.website-files.com/6272d3f738f67b4c8ee43a10/65a15680c5f22e9280143710_MTA%20Patient%20Survey%20Report%202024%20VF.pdf
Mill, R. C. (2008). Resorts: management and operation. John Wiley & Sons.
Mihalache, I. C. (2018). Medical tourism and its contribution to the development of economy. Revista Economica, 70(1).
Nelson, L. (April 13, 2015). Styling High Society at Elizabeth Arden’s Red Door Salon in Its Heyday. Vanity Fair. https://www.vanityfair.com/culture/2015/04/farm-to-fifth-avenue-elizabeth-arden-salon#:~:text=A%20few%20years%20prior%2C%20In%201909%2C%20she%20had,after%20her%20favorite%20the%20Tennyson
%20poem%2C%20%E2%80%9CEnoch%20Arden.%E2%80%9D
Norman, A., & Pokorny, J. J. (2017). Meditation retreats: Spiritual tourism well-being interventions. Tourism Management Perspectives, 24, 201-207.
Okumus, B., & Kelly, H. L. (2023). Wellness Management in Hospitality and Tourism. Goodfellow Publishers Ltd.
Olsen, D. H. (2016). Ritual journeys in North America: opening religious and ritual landscapes and spaces. International Journal of Religious Tourism and Pilgrimage, 4(1), 4.
Olsen, D. H., & Timothy, D. J. (Eds.). (2022). The Routledge handbook of religious and spiritual tourism. Abingdon, UK: Routledge.
Petrzela, N.M. (2023). Fit Nation: The Gains and Pains of America’s Exercise Obsession. University of Chicago.
Petropoulos, M. (2014). The cult and the use of Water in ancient Greece with emphasis on the ancient city of Patras. In Regional Symposium on Water, Wastewater and Environment: Traditions and Culture, e-Proceeding, Hellenic Open University, Patra (pp. 15-25).
Pocock, N. S., & Phua, K. H. (2011). Medical tourism and policy implications for health systems: a conceptual framework from a comparative study of Thailand, Singapore and Malaysia. Globalization and health, 7(12), 1-12.
Ponder, L.M. & Holladay, P. (2014). Yoga Tourism. In Encyclopedia of Tourism. Springer. 1-2
Pung, J., & Chiappa, G. (2020). An exploratory and qualitative study on the meaning of transformative tourism and its facilitators and inhibitors. European Journal of Tourism Research, 24, 2404-2404.
Pung, J. M., Gnoth, J., & Del Chiappa, G. (2020). Tourist transformation: Towards a conceptual model. Annals of Tourism Research, 81, 102885.
Risius,E. (n.d.). Why ‘Fat Camps’ Fail and Do Harm (And What to Do Instead). https://www.hhhealth.com/blog/why-fat-camps-fail-and-do-harm-and-what-to-do-instead/
Rodrigo, M. A. (2020). Spiritual tourism: Journey into the heart of the earth. Journal of Tourism and Leisure Studies, 4(2), 23.
Routh, H. B., Bhowmik, K. R., Parish, L. C., & Witkowski, J. A. (1996). Balneology, mineral water, and spas in historical perspective. Clinics in dermatology, 14(6), 551-554.
Scribner, V. (2016). The happy effects of these waters. Early American Studies, An Interdisciplinary Journal, 14(3).
Sheldon, P. J. (2020). Designing tourism experiences for inner transformation. Annals of Tourism Research, 83, 102935.
Shelton, F. H., White, J., Esterly, G., Minnick, J. P., Rex, G., Kennedy, S., Bones, J. & Burns, I. (1923). Springs and Spas of Old-Time Philadelphians. The Pennsylvania Magazine of History and Biography, 47(3), 196-237.
Smith, M. & Puczkó, L. (2014). Health, Tourism and Hospitality: Spas, Wellness and Medical travel. Routledge.
Soulard, J., McGehee, N. G., Stern, M. J., & Lamoureux, K. M. (2021). Transformative tourism: Tourists’ drawings, symbols, and narratives of change. Annals of Tourism Research, 87, 103141.
Spa Index. (2006, April 22).Thalassotherapy Spas in the USA. A guide to day spas and stay spas. https://www.spaindex.com/thalassotherapy-spas-in-the-usa/
Spivack, S. E. (1998). Health spa development in the US: A burgeoning component of sport tourism. Journal of Vacation Marketing, 4(1), 65-77.
Stein, T. J., Dev, C. S., & Tabacchi, M. H. (1990). Spas: Redefining the market. Cornell Hotel and Restaurant Administration Quarterly, 30(4), 46-52.
Stephano, R.M. (n.d.). Top 10 Medical Tourism Destinations in the World. Economics and Investment. Medical Tourism Magazine. https://www.magazine.medicaltourism.com/article/top-10-medical-tourism-destinations-world
Sterngass, J. (2001). First Resorts: Pursuing Pleasure at Saratoga Springs, Newport, and Coney Island. JHU Press.Stearns, N. D., Stearns, H. T., & Waring, G. A. (1937). Thermal springs in the United States (Vol. 679). US Government Printing Office.
Subbaraman, K., Singh, M., & Johar, I. P. (2021). Medical tourism: History, global scenario, and indian perspectives. In Growth of the Medical Tourism Industry and Its Impact on Society: Emerging Research and Opportunities (pp. 1-18). IGI Global.
Tackett, V. A. (1990). Visions of health: North American health resorts and their founders. The Union Institute.
Taylor, B. P. (1992). Our limits transgressed: Environmental political thought in America. University Press of Kansas.
Travel to Wellness. (n.d.). Wellness Tourism Association Introduces Industry Glossary. News and Noteworthy. https://www.traveltowellness.com/wellness-tourism-association-glossary/
Trimble, M. (2024, November 11). New-age spiritual retreats of the future. Vogue.https://www.vogue.com/article/new-age-spiritual-retreats-of-the-future
Tubergen, A., & Linden, S. (2002). A brief history of spa therapy. Annals of the rheumatic diseases, 61(3), 273-275.
Turrell, C. (2024, April 17). These sacred paths have attracted a new set of pilgrims: Fitness buffs. National Geographic. https://www.nationalgeographic.com/culture/article/pilgrimages-fitness-trend-walking-health
Urh, B. (2015). Healthy lifestyle and tourism. Quaestus, (6), 132.
Voigt, C., & Pforr, C. (2013). Wellness tourism: A destination perspective. In Routledge. Health and Wellness Tourism. A Focus on the Global Spa Experience. Routledge Media Company. https://www.routledge.com/rsc/downloads/Health_Wellness_Tourism_FB_final.pdf?srsltid=AfmBOoqqEjDM_xOaq3x8-CTDzVrLIqNY_dYZUm7uGXlKSTcXlU36jZbx
Weiss, T. (2004). Tourism in America before World War II. The Journal of Economic History, 64(2), 289-327.
Weissberg, E. (2023, May 17). They moved to a Buddhist retreat in rural America. Have they found happiness?. The Guardian. https://www.theguardian.com/us-news/2023/may/17/buddhism-arkansas-retreat-meditation-mindfulness
Willson, G. B., McIntosh, A. J., & Zahra, A. L. (2013). Tourism and spirituality: A phenomenological analysis. Annals of Tourism Research, 42, 150-168.
Wuthnow, R. (1985). The growth of religious reform movements. The annals of the American academy of political and social science, 480(1), 106-116.
Zollo, A., Simonetti, B., Salsano, V., & Rueda-Armengot, C. (2015). Promotion and marketing: Marketing strategies, Italy, regional development. In Health and wellness tourism: Emergence of a new market segment, 63-76.

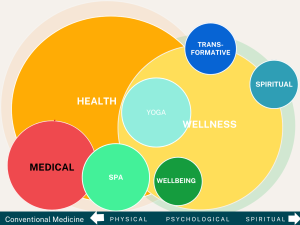
 Medical tourism, also known as medical travel, is defined as “contemporary travel for the primary purpose of obtaining indicated or elective dental or biomedical services” (Hudson & Li, 2012, p. 229). It is applied in the context of interstate, domestic, regional, or cross-border travel (including within the European Union) to receive medical, dental, or surgical care (Medical Tourism Association, 2024), though it is often used in an international context as well. According to the Medical Tourism Association, international medical tourism is now a $100 billion industry and is growing at a rate of 15% to 25% annually (2024).
Medical tourism, also known as medical travel, is defined as “contemporary travel for the primary purpose of obtaining indicated or elective dental or biomedical services” (Hudson & Li, 2012, p. 229). It is applied in the context of interstate, domestic, regional, or cross-border travel (including within the European Union) to receive medical, dental, or surgical care (Medical Tourism Association, 2024), though it is often used in an international context as well. According to the Medical Tourism Association, international medical tourism is now a $100 billion industry and is growing at a rate of 15% to 25% annually (2024). Health tourism is defined as “those types of tourism which have as a primary motivation the contribution to physical, mental, and/or spiritual health through medical and wellness-based activities” (European Travel Commission, 2018, p. 2). Thus, health tourism is an umbrella term that encompasses both medical and wellness tourism.
Health tourism is defined as “those types of tourism which have as a primary motivation the contribution to physical, mental, and/or spiritual health through medical and wellness-based activities” (European Travel Commission, 2018, p. 2). Thus, health tourism is an umbrella term that encompasses both medical and wellness tourism.

 Pilgrimage is a popular form of spiritual tourism. Pilgrimages are journeys undertaken by foot to sacred places, edifices or shrines, for a variety of reasons such as a deepened connection to faith, spiritual growth, healing, penance, or to demonstrate devotion. While the practice dates to ancient times, organized pilgrimages became particularly prominent in various religions, such as Christianity and Islam, around the early Middle Ages. Today, however, an increasing number of people are undertaking pilgrimages for personal rather than religious reasons. In 2023, nearly half a million people walked the Camino de Santiago in Spain, one of the most famous pilgrimage routes (Turrell, 2024). Data from the Camino de Santiago Bureau of Registration showed that only 40 % of walkers were doing so for religious reasons (Turrell, 2024). Many undertake the Camino for physical and mental health benefits, self-discovery, or simply to live in the moment while surrounded by the cultural, historical, and natural beauty of such ancient pathways (Turrell, 2024). Along with record foot traffic along established routes, new routes have opened across the globe from the United States to Ireland, Bhutan, and Sri Lanka (Turrell, 2024).
Pilgrimage is a popular form of spiritual tourism. Pilgrimages are journeys undertaken by foot to sacred places, edifices or shrines, for a variety of reasons such as a deepened connection to faith, spiritual growth, healing, penance, or to demonstrate devotion. While the practice dates to ancient times, organized pilgrimages became particularly prominent in various religions, such as Christianity and Islam, around the early Middle Ages. Today, however, an increasing number of people are undertaking pilgrimages for personal rather than religious reasons. In 2023, nearly half a million people walked the Camino de Santiago in Spain, one of the most famous pilgrimage routes (Turrell, 2024). Data from the Camino de Santiago Bureau of Registration showed that only 40 % of walkers were doing so for religious reasons (Turrell, 2024). Many undertake the Camino for physical and mental health benefits, self-discovery, or simply to live in the moment while surrounded by the cultural, historical, and natural beauty of such ancient pathways (Turrell, 2024). Along with record foot traffic along established routes, new routes have opened across the globe from the United States to Ireland, Bhutan, and Sri Lanka (Turrell, 2024). Wellbeing tourism is defined as travel “aiming to promote and maintain the health of the body, mind, and soul, while striving for a continuous state of balance and harmony” (Hjalager & Flagestad, 2012). It is closely related to wellness tourism but is distinguished primarily through its association with
Wellbeing tourism is defined as travel “aiming to promote and maintain the health of the body, mind, and soul, while striving for a continuous state of balance and harmony” (Hjalager & Flagestad, 2012). It is closely related to wellness tourism but is distinguished primarily through its association with 

 A 1938 Life Magazine article entitled, They Lose a Pound a Day the Milk Farm Way, highlighted the popularity of so-called milks farms. As a contemporary counterpart to the ‘health farm’ which catered to male, urban office workers in the habit of “slipping off for a couple of weeks of clean living and hard exercise”, milk farms targeted “stylish stouts” wanting to shed pounds from their “oversize figures” (Life, 1938, p.36).
A 1938 Life Magazine article entitled, They Lose a Pound a Day the Milk Farm Way, highlighted the popularity of so-called milks farms. As a contemporary counterpart to the ‘health farm’ which catered to male, urban office workers in the habit of “slipping off for a couple of weeks of clean living and hard exercise”, milk farms targeted “stylish stouts” wanting to shed pounds from their “oversize figures” (Life, 1938, p.36).
 A number of retreat centers in the US are hosted by Buddhist communities. The
A number of retreat centers in the US are hosted by Buddhist communities. The 